
Targeted Delivery of Chemotherapy and Immunotherapy: From Concept to Clinic
Cytotoxic chemotherapy and modern immunotherapies have transformed cancer care, but their benefits are limited by narrow therapeutic windows. Conventional drug dosing exposes large volumes of healthy tissue to toxic agents to reach a relatively small tumour mass. This mismatch drives much of the morbidity of treatment and, in some settings, prevents escalation to doses that would be required for maximal tumour control. Targeted drug delivery technologies attempt to invert this balance: concentrating drug at the tumour while sparing normal organs. Over the past two decades, a diverse portfolio of nanocarriers and biological vectors has moved from concept and patent space into animal studies, clinical trials and, in selected cases, routine practice.
Mechanistic Framework: Passive and Active Targeting
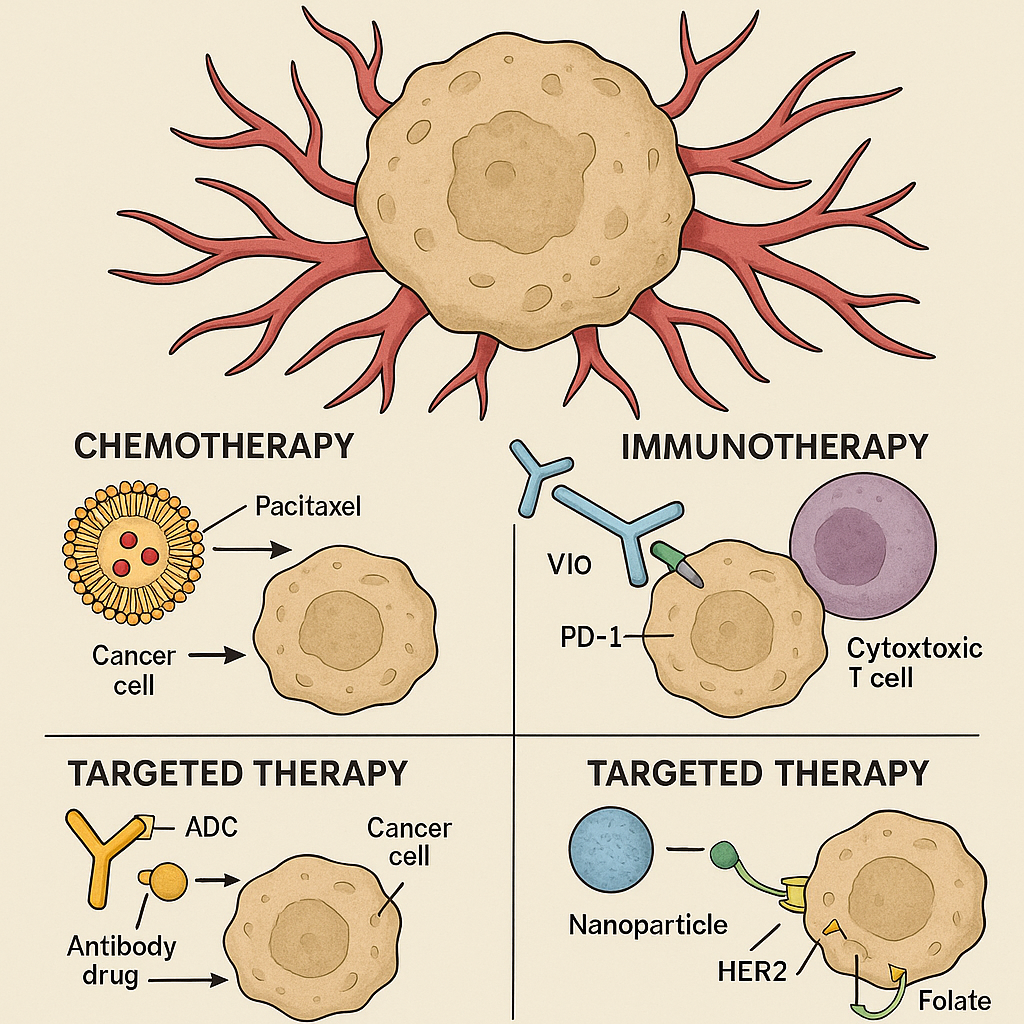
Most tumour-targeted systems exploit one of two broad mechanisms. Passive targeting relies on the “enhanced permeability and retention” (EPR) effect: abnormal, leaky vasculature and impaired lymphatic drainage in many solid tumours allow nanoscale particles (typically ≤ 200 nm) to extravasate and remain in the tumour interstitium more readily than in normal tissues. Polymeric nanoparticles, metallic particles (e.g. gold, iron oxide) and liposomes were originally designed to use this phenomenon, simply by tuning size and circulation half-life. Genexol-PM, a paclitaxel-loaded polymeric micelle, is a classic example that entered clinical use in parts of Asia by exploiting prolonged circulation and EPR-driven accumulation rather than explicit molecular targeting.
However, the EPR effect is heterogeneous between tumour types and between patients, and often modest in human disease compared with rodent models. Passive targeting alone therefore reduces off-target exposure but only partially solves the problem of specificity.
Active targeting adds a recognition step: ligands on the carrier surface bind cell-surface receptors that are overexpressed on tumour cells or tumour endothelium. Folic acid, RGD peptides, monoclonal antibodies and aptamers have all been used to decorate polymeric nanoparticles (e.g. PLGA-based systems), magnetic nanoparticles, gold nanoparticles, carbon nanotubes and quantum dots. By engaging receptors such as HER2, EGFR, or folate receptors, these carriers can be internalized more efficiently into malignant cells, increasing intracellular drug concentration while limiting uptake in normal tissues.
Beyond synthetic nanocarriers, biological vehicles have gained attention. Oncolytic viruses, engineered from HSV, adenovirus and others, preferentially replicate in and lyse tumour cells while igniting an anti-tumour immune response. Exosomes—30–120 nm extracellular vesicles produced by cells—offer a naturally occurring, biocompatible nanoparticle with inherent “homing” properties; exosomes derived from melanoma, for example, tend to traffic to lymph nodes, and exosomes from particular tissue lineages can cross otherwise formidable barriers such as the blood–brain barrier.
A complementary strategy is to design stimuli-responsive systems. These carriers remain relatively inert in circulation but release their payload in response to tumour-associated conditions such as acidic pH, specific enzymes, heat, or external triggers (ultrasound, light, magnetic fields). pH-sensitive liposomes and polymers, enzyme-cleavable linkers, and thermosensitive liposomes exemplify this approach.
Technologies in Established Clinical Use
Among the many platforms explored, two families have clearly crossed into routine oncology practice: liposomal formulations and antibody–drug conjugates (ADCs). A third, oncolytic virotherapy, has a first approved product in a narrow indication.
Liposomal and lipid-based formulations were the earliest nanocarriers to gain approval. Pegylated liposomal doxorubicin (Doxil/CAELYX) uses a stealth liposome to prolong circulation, exploit the EPR effect and reduce peak free-drug exposure. Across multiple trials in ovarian cancer, Kaposi’s sarcoma and metastatic breast cancer, these formulations generally achieved progression-free survival comparable to conventional doxorubicin but with substantially reduced cardiotoxicity and altered toxicity profiles (for example, hand–foot syndrome instead of heart failure). Pegylated liposomal irinotecan (Onivyde) combined with 5-fluorouracil and leucovorin improved overall survival in metastatic pancreatic cancer compared with standard therapy, demonstrating that for some agents, encapsulation can translate into both better tolerability and a meaningful survival benefit. Other approved liposomal formulations include DaunoXome (daunorubicin) and Marqibo (vincristine), used in Kaposi’s sarcoma and acute lymphoblastic leukaemia, respectively.
Antibody–drug conjugates represent the most mature form of “active” targeted chemotherapy. ADCs couple a monoclonal antibody against a tumour-associated antigen to a highly potent cytotoxic payload via a cleavable linker. After binding and internalization, the linker is degraded and the drug is released in the tumour cell or its microenvironment. First-generation ADCs such as gemtuzumab ozogamicin (Mylotarg) paved the way, and a second wave has followed with improved linker chemistry and payloads. Agents such as trastuzumab emtansine (T-DM1, Kadcyla) in HER2-positive breast cancer, brentuximab vedotin in CD30-positive lymphomas, sacituzumab govitecan in triple-negative breast cancer and enfortumab vedotin in urothelial carcinoma have demonstrated overall response rates in the 30–40% range in heavily pretreated populations, often with prolongation of progression-free survival and, in some cases, overall survival compared with physician’s-choice chemotherapy. Importantly, toxicity shifts from systemic myelosuppression to more target-linked patterns (e.g. neuropathy, interstitial lung disease), but cumulative burden is often lower than with unconjugated payloads.
Oncolytic virotherapy has one approved agent: talimogene laherparepvec (T-VEC), a modified HSV-1 expressing GM-CSF, for injectable melanoma lesions. In a phase III trial, T-VEC produced durable response rates significantly higher than GM-CSF alone, and durable remissions in a subset of patients. Its effect on overall survival is modest and limited to specific subgroups, but it provides proof-of-principle that local, immunogenic tumour lysis can meaningfully contribute to long-term control in some patients.
Collectively, these technologies have begun to reshape prognosis in selected niches: improving survival by months in aggressive diseases like metastatic pancreatic cancer, converting some advanced HER2-positive tumours into more chronic conditions, and, crucially, allowing patients to receive effective therapy with fewer debilitating side effects.
Emerging and Experimental Platforms
A large ecosystem of polymeric nanoparticles has demonstrated tumour accumulation and growth inhibition in animal models, including folate-decorated PLGA particles delivering docetaxel or other cytotoxics. Systematic patent reviews indicate a very high level of activity around polymeric, metallic, silica, lipid, albumin-based and quantum-dot carriers for oncology. Yet, apart from a few regionally approved products such as Genexol-PM, most remain in early-phase clinical trials. In humans, these systems have so far tended to match conventional regimens in efficacy while reducing certain toxicities, but robust, reproducible survival gains across tumour types have not yet materialized.
Gold nanoparticles illustrate the gap between preclinical promise and clinical reality. In rodent models, gold nanostructures can serve as drug carriers or photothermal agents, achieving high tumour accumulation and local ablation with externally applied near-infrared light. Early human studies with constructs such as CYT-6091 (TNF-decorated gold nanoparticles) and silica–gold nanoshells for prostate tumour ablation have shown acceptable safety and technical feasibility. However, concerns about long-term biodistribution, organ retention and manufacturability have so far prevented mainstream therapeutic approval.
Stimuli-responsive systems have reached the clinic largely through the example of ThermoDox, a heat-sensitive liposomal doxorubicin intended to release its payload when tumours are heated by radiofrequency ablation. Despite encouraging preclinical data, phase III trials in hepatocellular carcinoma failed to show significant improvement in progression-free or overall survival compared with ablation alone, underscoring the challenge of controlling in vivo triggers precisely enough to gain a consistent therapeutic advantage.
Exosome-based delivery is at an even earlier stage. In mouse models, exosomes loaded with chemotherapeutics or siRNA against oncogenic drivers (e.g. KRAS) have improved drug distribution to tumours and suppressed growth. Their ability to cross biological barriers and evade immune detection makes them highly attractive carriers conceptually, and first-in-human phase I studies are underway. Yet significant hurdles in scalable production, purification and cargo control must be solved before exosomes can realistically alter patient prognosis.
Finally, hybrid and magnetically guided systems—such as composite PLGA–magnetic– albumin nanoparticles guided to tumours by external magnets and protected by intellectual property like US Patent US2012/0265001—represent clever engineering solutions that remain largely in the patent and preclinical domains.
Prognostic Impact and Future Directions
When viewed across the whole field, targeted delivery has unquestionably improved the quality of cancer treatment. Liposomes and ADCs have allowed clinicians to deliver active drugs to frail or heavily pretreated patients who could not tolerate conventional regimens. In some indications, such as metastatic pancreatic cancer with liposomal irinotecan combinations or HER2-positive breast cancer with successive lines of ADCs, median overall survival has improved by several months compared with earlier standards. For many patients, this translates into more time with preserved function and fewer hospitalizations.
At the same time, the magnitude of survival benefit attributable purely to drug delivery technology is often modest. Tumour biology, resistance mechanisms, and host factors still dominate long-term prognosis. EPR heterogeneity, variable target expression, and adaptive resistance limit how far improved pharmacokinetics can be converted into durable remissions. Moreover, the complexity and cost of many advanced carriers restrict global access and pose challenges for large-scale manufacturing.
The most promising trajectory likely lies in integration: using targeted carriers to deliver not only cytotoxics but also immunomodulators, nucleic acids and multi-drug combinations; combining oncolytic viruses and exosomes with checkpoint inhibitors; and embedding biomarker-driven patient selection into trial design. In that context, targeted chemotherapy and immunotherapy delivery will be less a standalone solution and more a backbone technology enabling more precise, adaptable and tolerable cancer treatment.
References (selected)
- Hazis M, et al. Systematic Patent Review of Nanoparticles in Drug Delivery and Cancer Therapy in the Last Decade.
- Madej M, et al. Polymeric Nanoparticles—Tools in a Drug Delivery System in Selected Cancer Therapies. Appl Sci. 2022.
- Gatto L, et al. Targeted Liposomal Drug Delivery: Overview of Current Applications and Challenges. Life. 2024.
- Fu Z, et al. Antibody–Drug Conjugate: The “Biological Missile” for Targeted Cancer Therapy. Signal Transduct Target Ther. 2022.
- Omolekan M, et al. Viral Warfare: Unleashing Engineered Oncolytic Viruses to Outsmart Cancer’s Defenses. Front Immunol. 2025.
- Palakurthi S, et al. A Comprehensive Review of Challenges and Advances in Exosome-Based Drug Delivery Systems. Nanoscale Adv. 2024.
- Torres L, et al. Innovations in Cancer Therapy: Endogenous Stimuli-Responsive Liposomes as Advanced Nanocarriers. Pharmaceutics. 2025.
- Bhattacharya S, et al. pH- and Stimuli-Responsive Polymeric Nanoparticular Systems to Improve Drug Delivery in Cancer Therapy. Crit Rev Oncol Hematol. 2023.
- Prajapati N, et al. Receptor-Targeted Nanomedicine for Cancer Therapy. Receptors. 2024.
- US Patent US2012/0265001A1. Composite Magnetic Nanoparticle Drug Delivery System.